Ovarian Cancer Prevention
Can ovarian cancer be prevented?
Several approaches may be used to lower the risk for ovarian cancer in high-risk people. Each approach differs in their benefits, risks and effectiveness. None of these approaches completely eliminates the risk for cancer.
- Medications can lower the risk for ovarian cancer, but enough risk remains that experts may still recommend surgery.
- Risk-reducing surgery to remove the ovaries and is the most effective way to lower risk in high-risk people.
The decision to have surgery or take medication to lower your risk is deeply personal. Speak with a genetic counselor and a gynecologic surgeon to understand your risks for cancer and preventive options.
Can medications lower the risk for ovarian cancer?
Combined hormonal contraceptives (pills, patch, ring) containing both and progesterone may reduce the risk for ovarian cancer both in people of average risk and those who are at high risk due to an .
If you are interested in taking hormonal contraceptives to lower your risk for ovarian cancer, you should discuss the benefits, risks and limitations with your healthcare provider.
Can surgery lower the risk for ovarian cancer?
Different types of surgery may be used to lower the risk for ovarian cancer.
- Removal of the ovaries and (salpingo-oophorectomy) is the most effective way to lower risk for ovarian cancer.
- Removal of the only () may also lower the risk for ovarian cancer.
You can read more about each surgery below.
Surgery can have risks and side effects. It's important for people to speak with experts in order to learn as much as possible about their endometrial cancer risk and to make an informed decision about the best option for lowering their risk.
What is risk-reducing salpingo-oophorectomy?
Risk-reducing salpingo-oophorectomy () refers to the removal of the healthy ovaries and to reduce a person's risk of developing cancer. Decades of research on in high-risk individuals has shown that:
- It is an effective way to lower the risk for ovarian and cancer. It does not completely eliminate the risk for these cancers. There is a remaining risk for primary peritoneal cancer even after the ovaries and tubes have been removed, but this risk is very small.
- It can lower the risk for death in high-risk women.
- It may also lower the risk for breast cancer in certain high-risk women.
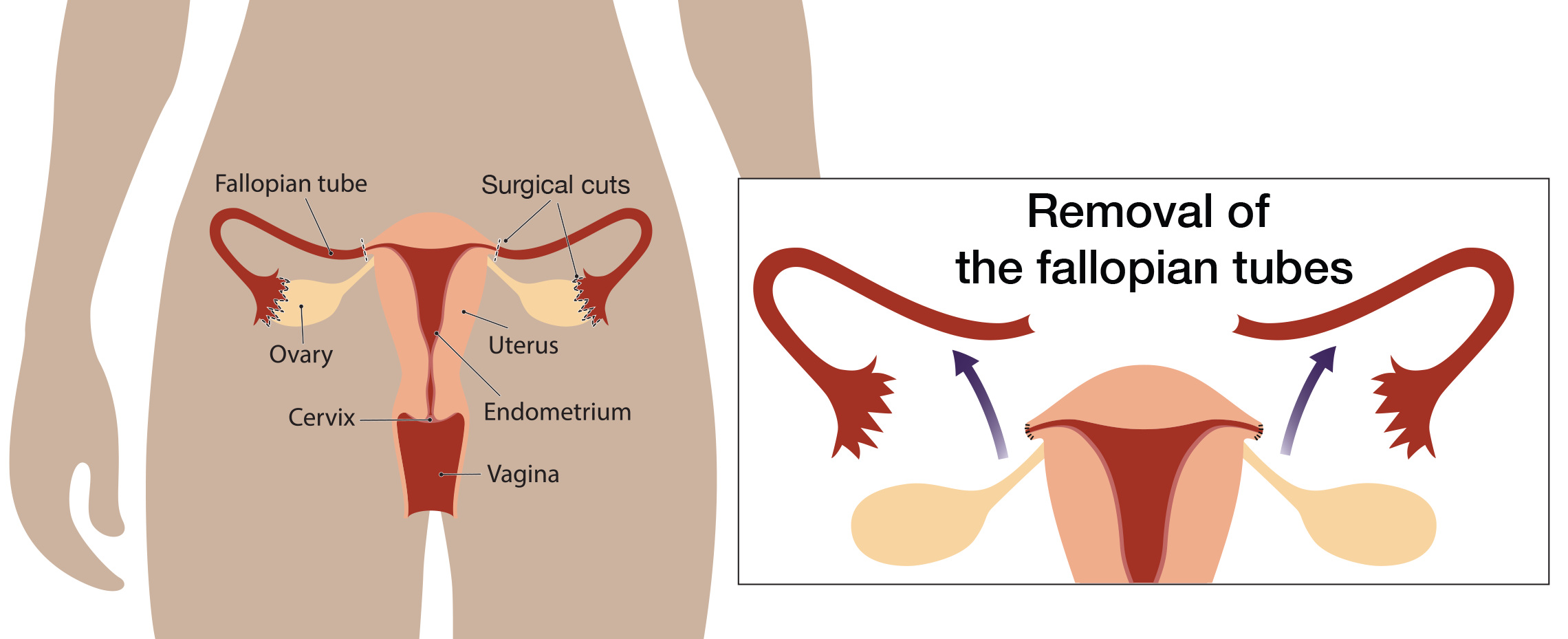
What is risk-reducing salpingectomy?
involves removal of the only. Research suggests that the may be the source of many ovarian cancers. This has led researchers to study if it is safe to remove the only before menopause and delay removal of the ovaries until after menopause.
Studies looking at to lower risk are currently enrolling people. Until these studies are completed, experts cannot say for certain that lowers the ovarian cancer risk in high-risk people.
may be an option for high-risk women who are not ready to remove their ovaries. Experts recommend that women who decide to have surgery to remove their tubes alone follow up with a second surgery to remove their ovaries (known as completion ) as soon as they are ready.
Should I have a hysterectomy?
Hysterectomy (removal of the uterus) may be performed at the same time as removal of the ovaries and tubes. People often ask if they should remove their uterus at the time of risk-reducing ovarian surgery. Here are some factors that might affect the decision to have a hysterectomy at the time of surgery to remove the ovaries and tubes:
- Increased risk for both ovarian and uterine cancer. This includes people with mutations in the genes. Although the overall risk is very small, some studies have linked an inherited to a very rare but aggressive type of . Medications like tamoxifen and progesterone may also increase the risk for uterine cancer. Visit our section on for more information about these risks.
- Previous abnormal pap smears or any abnormality of the uterus.
- Considerations about hormone replacement. Hysterectomy in order to simplify hormone replacement. There is an increased risk for uterine cancer in women who take alone compared to with progesterone. Women who have hysterectomy can take without progesterone. alone may have fewer side effects than with progesterone. See our section on Surgical Menopause for more information.
- Additional surgical risk of hysterectomy. Removing the uterus involves more surgery than alone. There is a slight increase in the risk for complications and the possibility that a laparoscopic procedure will turn into a full abdominal surgery.
- Insurance coverage. Because of the surgery, recovery and hospitalization are lengthier; some insurance companies won’t pay for hysterectomy unless there is medical necessity.
- Possible long term effects of hysterectomy. Hysterectomy has been linked to urinary leakage (incontinence) and bladder prolapse due to weakening of the pelvic muscles.
Visit our Tip-Sheet Wizard page for a tool to help you ask questions and make an informed decision about whether or not to have a hysterectomy.
Get notified when updated information becomes available.
SIGN UP FOR CONTENT UPDATES
Topic : Reducing ovarian cancer risk without removing the ovaries
A leading ovarian cancer organization has recommended that all women who have pelvic surgery...

Study : Endometrial cancer risk for people with BRCA1 and BRCA2 mutations
This study looked at how often endometrial cancer occurred in people with...
Laparoscopic surgery
In the past, risk-reducing removal of the ovaries and tubes were performed using open surgery (also known as a laparotomy). This involves one long incision in the lower abdomen to remove the ovaries and , (and for those undergoing hysterectomy, the uterus).
Today, risk-reducing removal of the ovaries and tube can usually be performed by laparascopic surgery (also known as minimally-invasive surgery). Laparoscopic surgery involves a small incision made in the abdomen to insert a flexible scope with a camera, which is used to see the ovaries and tubes. Addition small incisions are made to insert surgical instruments needed to remove the ovaries and tubes.
In general, people who have surgery by laparoscopy may heal quicker and spend a shorter time in the hospital than people who have open surgery.
Surgical risks and recovery
Every surgery has risks; some are more serious than others. Some risks can affect recovery or long term health
- Infection
- Delayed healing
- Blood loss
- Blood clots
- Pain (post-operative and long term pain syndromes)
- Surgical menopause and related health issues (see our section on Side Effects of Menopause for more information)
- Injury to internal organs
- Bladder incontinence
- Sexual side effects
It is important for people to discuss possible surgical risks with a surgeon to understand the seriousness and likelihood of these risks before making the decision to have risk-reducing surgery.
Average recovery time after is about 1-2 weeks. Recovery after open surgery is longer, up to 6 weeks.
Who should have risk-reducing removal of the ovaries and tubes?
The National Comprehensive Cancer Network (NCCN), is an organization of cancer experts that creates guidelines on cancer care and updates them yearly. NCCN's guidelines include recommendations for risk-reducing salpingo-oophorectomy based on an individual's gene mutation and situation. Each gene has a slightly different recommendation, click on the links for each gene for the full risk-management recommendation.
|
Gene |
Beginning Age |
Recommendation |
|
35-40 |
The guidelines recommend risk-reducing removal of ovaries and (). Timing of surgery should take into account plans to have children. Removal of only the () is an option for people who are not ready to remove their ovaries. At this time, it is not known if is effective for lowering the ovarian cancer risk in high-risk people. People who choose should have a completion to lower their remaining risk for ovarian cancer when they are ready. |
|
|
40-45 |
||
|
45-50 |
The guidelines recommend risk-reducing removal of ovaries and (). Timing of surgery should take into account plans to have children. Removal of only the () is an option for people who are not ready to remove their ovaries. At this time, it is not known if is effective for lowering the ovarian cancer risk in high-risk people. People who choose should have a completion to lower their remaining risk for ovarian cancer when they are ready. |
|
|
45-50 |
The guidelines state that people with mutations in should consider risk-reducing salpingo-oophorectomy. This involves having a conversation with your doctor to decide if the benefits of surgery outweigh the risks. The timing of surgery should take into account plans to have children. Removal of only the () is an option for people who are not ready to remove their ovaries. At this time, it is not known if is effective for lowering the ovarian cancer risk in high-risk people. People who choose should have a completion to lower their remaining risk for ovarian cancer when they are ready. |
|
|
No set age |
More research is needed to determine whether people with mutations in benefit from risk-reducing surgery to remove their ovaries and . Currently, experts recommend that you have a discussion with your doctor about the benefits and risks of surgery taking into account your family history of gynecologic cancer. Removal of only the () is an option for people who are not ready to remove their ovaries. At this time, it is not known if is effective for lowering the ovarian cancer risk in high-risk people. |
|
|
40 |
The guidelines state that people with mutations in these genes should consider risk-reducing salpingo-oophorectomy. This involves having a conversation with your doctor to decide if the benefits of surgery outweigh the risks. The timing of surgery should take into account plans to have children. Removal of only the () is an option for people who are not ready to remove their ovaries. For people planning risk-reducing hysterectomy, the tubes should be removed at the same time. |
|
|
40 for at the time of hysterectomy 50 for salpingo-oophorectomy |
More research is needed to determine whether people with mutations in benefit from risk-reducing surgery to remove their ovaries. Currently, experts recommend that you have a discussion with your doctor about the benefits and risks of surgery taking into account your family history of gynecologic cancer. Removal of only the () is an option for people who are not ready to remove their ovaries. For people planning risk-reducing hysterectomy, the tubes should be removed at the same time. |
|
|
50 |
More research is needed to determine whether people with mutations in benefit from risk-reducing surgery to remove their ovaries and . Currently, experts recommend that you have a discussion with your doctor about the benefits and risks of surgery taking into account your family history of gynecologic cancer. Removal of only the () is an option for people who are not ready to remove their ovaries. For people planning risk-reducing hysterectomy, the tubes should be removed at the same time. |
|
|
Source: NCCN Guidelines: Genetic/Familial High-Risk Assessment: Breast, Ovarian, Pancreatic, , vs. 2, 2026; Source: NCCN Guidelines: Genetic/Familial High-Risk Assessment: Colorectal, Endometrial, Gastric vs. 1, 2025. |
||



Visit our Partners
Ovarian Cancer Research Alliance
Dedicated to fighting ovarian and all gynecologic cancers on all fronts while supporting patients and their families.
SHARE Cancer Support
Support and education resources in English and Spanish for people affected by ovarian cancer.
National Ovarian Cancer Coalition
Saving lives through the prevention and cure of ovarian cancer and by improving the quality of life for survivors and their caregivers.