Study: Risk-reducing ovarian cancer surgery and quality of life
Summary
People with an inherited BRCA gene mutation are recommended to have surgery to remove their ovaries before the age of natural menopause to reduce their risk of ovarian cancer. This surgery can cause short-term and long-term effects. This study assesses the quality of life among people who have their fallopian tubes surgically removed and later have their ovaries removed compared to people who have their ovaries and fallopian tubes removed at the same time. (Posted 7/26/22). Este artículo está disponible en español.

Relevance
This article is most relevant for People with an inherited BRCA mutation
Relevance: Medium-High

Strength of Science: High
Research Timeline: Human Research

Media Ratings
Did you see the media coverage of this article?
Who covered this study?
cancernetwork
Risk-Reducing Salpingectomy Yields Higher QoL for BRCA1/2 Pathogenic Variant Carriers With Gynecologic Cancer


![]() This article rates 3.5 out of 5 stars
This article rates 3.5 out of 5 stars
Contents
| At a glance | Guidelines |
| Study findings | Questions for your doctor |
| Strengths and limitations | Clinical trials |
| What does this mean for me? | Related resources |
STUDY AT A GLANCE
What is this study about?
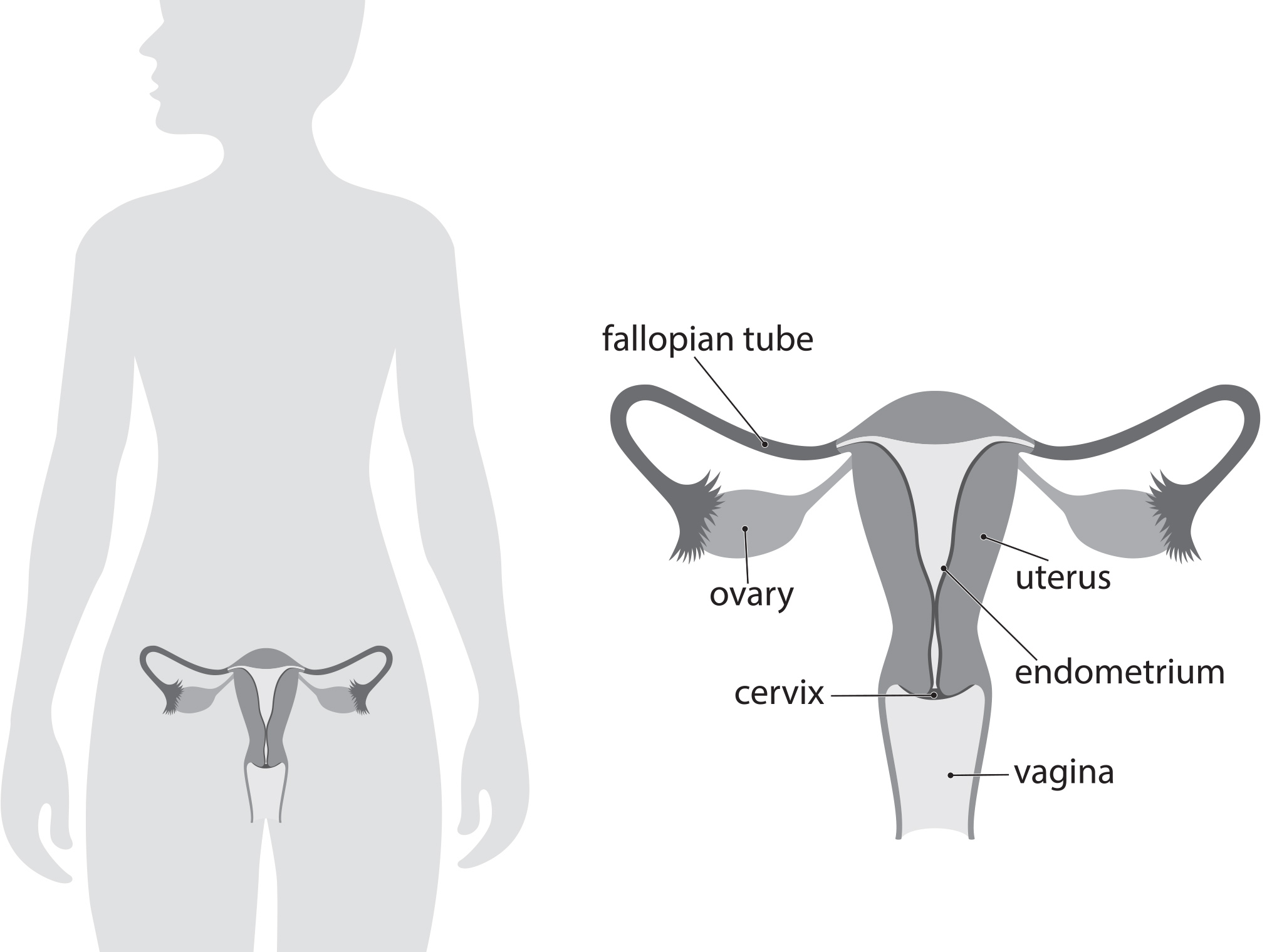
This study is about menopause-related quality of life in people with an inherited mutation who had surgery to reduce their ovarian cancer risk. The researchers compared people who first removed their only (risk-reducing or RRS) and later removed their ovaries to people who had their and ovaries removed at the same time (risk-reducing salpingo-oophorectomy or ). See image of reproductive tract below.
Why is this study important?
Current guidelines recommend (removal of the ovaries and ) for people with an inherited mutation—between ages 35-40 for and ages 40-45 for –who have completed childbearing. However, risk-reducing removal of the ovaries at these ages results in early menopause and may lead to related short-term (hot flashes, sleep disturbances, impaired sexual function and others) and long-term (possible risk of heart disease, , impairment and others) effects.
Experts believe that the most common type of ovarian cancer usually begins in the . This knowledge shift regarding where ovarian cancer begins has led to the possibility that risk-reducing removal of the followed by delayed removal of the ovaries could lower cancer risk while postponing menopause and the associated side effects.
Study findings
A total of 577 people participated in this study, with an average age of 37. Among these participants:
- 297 had a mutation.
- 280 had a mutation.
- 394 patients had RSS (removal of )
- 154 had (removal of both and ovaries)
Quality of life, sexual distress and functioning were measured at three months and again at one year after surgery.
- Reported quality of life was better among participants who only had their removed (RSS) compared to participants who had their and ovaries removed (RSSO) in a single procedure.
- Comparatively, patients who had RRS reported a better quality of life, even when patients who had used hormone replacement therapy.
- People who chose reported more impaired sexual function after their surgery compared to those who chose RRS with delayed RRO.
- People who chose reported more sexual distress after their surgery compared to those who chose RRS with delayed RRO.
Overall, patients have better menopause-related quality of life after RRS than after . In this study, this was true regardless of whether or not a patient took hormone replacement therapy. Even though patients who used hormone replacement therapy after had worse symptoms than patients who chose RRS, using hormonal replacement therapy after did reduce the severity of symptoms after compared to patients who did not use hormone replacement after .
Strengths and limitations
Strengths
- This was a study conducted at all university hospitals and some general hospitals in the Netherlands. Patients were followed up at 3 and 12 months after surgery.
- A large number of participants were included in the study, many of whom chose RRS with delayed RRO.
Limitations
- The study was not designed to show whether people who chose had a lower risk for developing ovarian cancer compared with people who chose RRS with delayed RRO. We still do not yet know if RRS with delayed RRO is as effective as for reducing ovarian cancer risk. Another study known as SOROCk is looking at this outcome but will not have results for at least another 10 years.
- Participants chose which surgery they preferred (RRS with delayed RRO or ). Patient preference may have biased the results.
What does this mean for me?
Current guidelines recommend risk-reducing removal of the ovaries and () between ages 35-40 for mutation carriers and ages 40-45 for mutations carriers upon completion of childbearing.
This study in the Netherlands found that patients with a mutation have better menopause-related quality of life after an RSS than an . (RSS is not standard of care in the US.) A similar study called WISP (which is no longer enrolling participants) is being conducted in the US. A much larger, longer-term study called SOROCk is currently enrolling mutation carriers in the US. The goal of SOROCk is to learn if RRS with delayed RRO lowers ovarian cancer risk as safely and effectively as .
Reference
Steenbeek MP, Harmsen MG, Hoogerbrugge N, et al. Association of With Delayed Versus Salpingo-oophorectomy With Quality of Life in BRCA1/2 Pathogenic Variant Carriers: A Nonrandomized Controlled Trial. JAMA Oncol. 2021;7(8):1203–1212.
Disclosure: FORCE receives funding from industry sponsors, including companies that manufacture cancer drugs, tests and devices. All XRAYS articles are written independently of any sponsor and are reviewed by members of our Scientific Advisory Board before publication to assure scientific integrity.
Share your thoughts on this XRAY review by taking our brief survey.
posted 7/26/22
This article is relevant for:
People with an inherited BRCA mutation
This article is also relevant for:
previvors
people with a genetic mutation linked to cancer risk
Be part of XRAY:
IN-DEPTH REVIEW OF RESEARCH
Study background
People with an inherited mutation have a 40-60 percent lifetime risk of ovarian cancer, while people with an inherited mutation have a lifetime risk of 15-30 percent.
Risk-reducing salpingo-oophorectomy () significantly lowers the risk of ovarian cancer but has several disadvantages. induces premature menopause with potential short-term (hot flashes, sleep disturbances, impaired sexual function) and long-term (risk of cardiovascular disease, , impairment) side effects.
High-grade serous cancer, the most common type of ovarian cancer, is believed to frequently originate in the . This paradigm shift supports risk-reducing (RRS) with delayed (RRO) as a novel risk-reducing strategy that postpones menopause and its related side effects. However, no data on quality of life (QoL) nor on cancer risk reduction from RRS has been reported.
Researchers of this study wanted to know
The researchers wanted to assess the menopause-related quality of life in mutation carriers after removal of their (RRS) followed by delayed removal of their ovaries (RRO) compared to standard (simultaneous removal of the and ovaries).
Populations looked at in this study
A total of 577 people from the Netherlands participated in this study. The average age of participants was 37. Of these:
- 297 (51.5%) had a mutation.
- 280 (46%) had a mutation.
- 413 (71.6%) chose RRS with delayed RRO.
- 394 had the surgery.
- 164 chose RRSO
- 154 had the surgery.
- Most (87%) had children as well as a medium-to-high level of education.
- Some (14%) had a with ovarian cancer.
- Some (14%) had a personal history of breast cancer.
- Many (60%) had risk-reducing mastectomy.
Study design
Participants chose the type of risk-reducing surgery (RRS or ) they would undergo.
- 394 patients had RSS
- RRS was occasionally combined with hysterectomy (n=1) or breast surgery (n=4).
- 154 had RRSO
- was occasionally combined with hysterectomy (n=5) or breast surgery (n=14).
Study findings
The study’s primary outcome was quality of life (QoL). This was measured at baseline, three months, and one year after surgery using the Greene Climactic Scale (the period of life starting from the decline in ovarian activity until after the end of ovarian function). Participants then completed a biennial questionnaire measuring 21 menopause-related symptoms on a four-point scale. The three areas measured included depression/anxiety, vasomotor (hot flashes and night sweats) and sexual problems.
Secondary data was collected on sexual function, using two web-based questionnaires: the Female Sexual Functioning Index and the Female Sexual Distress Scale.
Follow-up on cardiovascular disease and cost-effectiveness has not been completed.
Quality of Life outcomes
- Patient-reported quality of life was better among participants who only had their removed (RSS) compared to participants who had their and ovaries removed (RSSO).
- Without hormone replacement therapy the mean increase from the Greene baseline score was 6.7 points higher during 1 year after than after RRS.
- After with hormone replacement therapy, the difference was 3.6 points higher compared to RRS.
- These findings were similar at 3 months and 1 year after surgery and on all subsequent time points.
- Hot flashes, sudden excitability, irritability and loss of sexual interest were the most frequently reported symptoms.
Sexual Distress and Functioning
- People who chose , whether or not they used hormone replacement therapy, reported more impaired sexual functioning after their surgery compared to those who chose RRS with delayed RRO. However, if participants used hormone replacement therapy after , their sexual functioning was not as severely affected as participants who did not use hormone replacement after .
- In the RRS group, impaired sexual functioning was reported by 121 of 388 participants (31%) at baseline, which remained relatively similar over time (28% at 3 months and 1 year).
- Impaired sexual functioning was reported in 53 of 148 participants (36%) in the group at baseline, which increased over time (44% at 3 months and 56% at 1 year).
- The authors did not provide the specific rates of impaired sexual functioning in the group for people who used hormone replacement therapy after surgery versus people who did not use hormone replacement after surgery.
- People who did not use hormone replacement therapy after had a worsening in their sexual function score of 5.7 points more than those who chose RRS, whereas people who used hormone replacement therapy after had a worsening in their sexual function score of only 2 points more than those who chose RRS. This suggests that although people who chose , whether or not they used hormone replacement therapy, had worse impaired sexual functioning after their surgery compared to those who chose RRS with delayed RRO, the worsening in sexual functioning observe in participants who used hormone replacement therapy after was not as severe as that seen in participants who did not use hormone replacement after .
- Regardless of reported sexual functioning, participants who chose RRS experienced less sexual distress than participants who chose and did not use hormone replacement therapy. Levels of sexual distress after surgery were similar for participants who chose RRS and participants who chose and used hormone replacement therapy.
- Sexual distress was reported by 69 of 388 participants (18%) at baseline, which remained relatively constant over time (19% at 3 months and 18% at 1 year).
- Sexual distress was reported by 34 of 149 participants (23%) in the group at baseline, which increased over time (32% at 3 months and 42 % at 1 year).
- Participants in the group who used hormone replacement therapy after surgery did NOT have increased levels of sexual distress after surgery compared to participants in the RRS group. Only participants in the group who did not use hormone replacement therapy after surgery experienced more sexual distress.
- A similar decline in cancer worry was observed after RRS and regardless of hormone replacement use.
- No significant difference in a participant’s decision (conflict or regret) was found.
Strengths and limitations
Strengths
- This was a study done at all university hospitals and some general hospitals in the Netherlands. Patients were followed up at 3 and 12 months after surgery.
- This study included a large number of participants, many of whom chose RRS with delayed RRO.
Limitations
- The main limitation of this study was that it was not . Participants chose the type of surgery they would have (RRS with delayed RRO versus ). Patient preference may have biased the results.
- The study was not designed to show whether people who chose had a lower risk for developing ovarian cancer compared with people who chose RRS with delayed RRO. We still do not yet know if RRS with delayed RRO is as effective as for reducing ovarian cancer risk. A study known as SOROCk is looking at that outcome but it will not have results for at least 10 years.
Context
Two previous studies reported that 34-44 percent of mutation carriers were interested in postponing premature menopause. This is the first study to compare the menopausal-related quality of life after RRS with delayed RRO and . (The WISP study being conducted in the US is similar but is no longer enrolling participants.)
While RRS with delayed RRO improves quality of life, it has potential drawbacks, including increased worry about developing cancer, regret about surgical decisions and surgical complications. Currently, how RRS with delayed RRO decreases cancer risk is unknown.
Conclusions
In this study, patients who had RRS reported better menopause-related quality of life and better sexual functioning compared to patients who had . This was true whether participants took hormone replacement therapy, although using hormone therapy helped improved some aspects of sexual functioning. A large international follow-up study (TUBA-WISP-II) is looking at cancer outcomes in people who have RRS with delayed RRO.
Share your thoughts on this XRAY review by taking our brief survey.
posted 7/26/22
 Expert Guidelines
Expert Guidelines
The National Comprehensive Cancer Network (NCCN) provides guidelines for management of gynecologic cancer risk in people with and mutations.
Prevention
- Risk-reducing removal of ovaries and , (known as salpingo-oophorectomy) is recommended between ages 35-40 for and 40-45 for and upon completion of childbearing.
- Research studies show that removing the ovaries can increase survival for women with mutations.
- Women should talk with their doctors about the effects of early menopause and options for managing them.
- Women should talk with their doctors about the risks and benefits of keeping or removing their uterus (hysterectomy), including:
- Women with a mutation have an increased risk for a rare form of aggressive uterine cancer; hysterectomy removes this risk.
- For women considering hormone replacement after surgery, the presence or absence of a uterus can affect the choice of hormones used.
- Estrogen-only hormone replacement is less likely to increase the risk for breast cancer, although it increases the risk for uterine cancer. Women who still have their uterus are typically given hormone replacement with both and progesterone.
- Adding progesterone to hormone replacement can protect against uterine cancer. However, the combination of these hormones may increase the risk for breast cancer more than alone.
- A medical history of fibroids or other uterine or cervical issues may justify a hysterectomy.
- Oral contraceptives (birth control pills) have been shown to lower the risk for ovarian cancer in women with mutations. Research on the effect of oral contraceptives on breast cancer risk has been mixed. Women should discuss the benefits and risks of oral contraceptives for lowering ovarian cancer risk with their doctors.
- Removal of the only () is being studied as an option for lowering risk in high-risk women who are not ready to remove their ovaries. Studies on the effects of are ongoing. At this time whether lowers the risk for ovarian cancer in high-risk women remains unknown.
- Consider enrolling in a research study looking at this procedure to lower cancer risk.
Screening
- There are no proven benefits to routine ovarian cancer screening using transvaginal and a blood test. However, some doctors still recommend this screening, starting at ages 30-35.
- Women should be aware of the symptoms of gynecologic cancer and report abnormalities to their doctors.
Updated: 08/06/2022
 Questions To Ask Your Doctor
Questions To Ask Your Doctor
- Am I a candidate for RRS followed by delayed RRO to reduce my ovarian cancer risk?
- Do you recommend hormone replacement therapy after ?
- Are there other ways to reduce my menopausal symptoms after instead of or in addition to hormone replacement therapy?
- Are there other ways to lower my risk for ovarian cancer?
 Open Clinical Trials
Open Clinical Trials
The following are studies looking at ovarian cancer screening or prevention.
- NCT04251052: A Study to Compare Two Surgical Procedures in Women with Mutations to Assess Reduced Risk of Ovarian Cancer (SOROCk). This study is looking at whether women with mutations who remove just the can reduce the risk of ovarian cancer nearly as much as women who remove their ovaries and .
- NCT05287451: Risk Reducing With Delayed as an Alternative to Risk- Reducing Salpingo-oophorectomy in High Risk-Women to Assess the Safety of Prevention. This study will look at outcomes in women with , , , and who remove their , followed by removal of their ovaries compared to women who undergo standard-of-care removal of their ovaries and at the same time.
- Validating a Blood Test for Early Ovarian Cancer Detection in High-risk Women and Families: MicroRNA Detection Study (MiDE). The goal of MiDe is to develop a test to detect early-onset ovarian cancer. Currently, no reliable screening or early detection tests are available. Participants can be expected to provide up to 4 tubes of blood every 6 months for up to 5 years. These samples can be collected by mobile phlebotomy all around the US.
- NCT04794322: Developing a Test for the Detection of Ovarian Cancer. This study aims to develop an ovarian cancer early detection test that looks at found in a uterine (womb) washing and proteins found in the blood. Participants will not receive the results of their tests.
Additional clinical trials for ovarian cancer screening and prevention may be found here.
Updated: 09/11/2022
 Peer Support
Peer Support
FORCE offers many peer support programs for people with inherited mutations.
- Our Message Boards allow people to connect with others who share their situation. Once registered, you can post on the Diagnosed With Cancer board to connect with other people who have been diagnosed.
- Our Peer Navigation Program will match you with a volunteer who shares your mutation and situation.
- Our moderated, private Facebook group allows you to connect with other community members 24/7.
- Check out our virtual and in-person support meeting calendar.
- Join one of our Zoom community group meetings.
Updated: 08/06/2022
 Related Resources
Related Resources
The following organizations have resources related to ovarian cancer.
- FORCE resources:
- Information: Ovarian cancer screening and prevention
- Information: Ovarian cancer treatment
- Personalized portal: Ovarian cancer
- XRAY category: Ovarian cancer
- Video: What's new in gynecologic cancer screening and prevention?
- Video: What's new in gynecologic cancer treatment?
- Video: Options for Ovarian Cancer
- Video playlist: Ovarian cancer
- Blogs: Ovarian cancer
- National Comprehensive Cancer Network Guidelines for Patients: Ovarian Cancer
- National Ovarian Cancer Coalition
- Ovarian Cancer Research Alliance
- Clearity Foundation
Updated: 06/28/2023
Who covered this study?
cancernetwork
Risk-Reducing Salpingectomy Yields Higher QoL for BRCA1/2 Pathogenic Variant Carriers With Gynecologic Cancer ![]() This article rates 3.5 out of 5 stars
This article rates 3.5 out of 5 stars